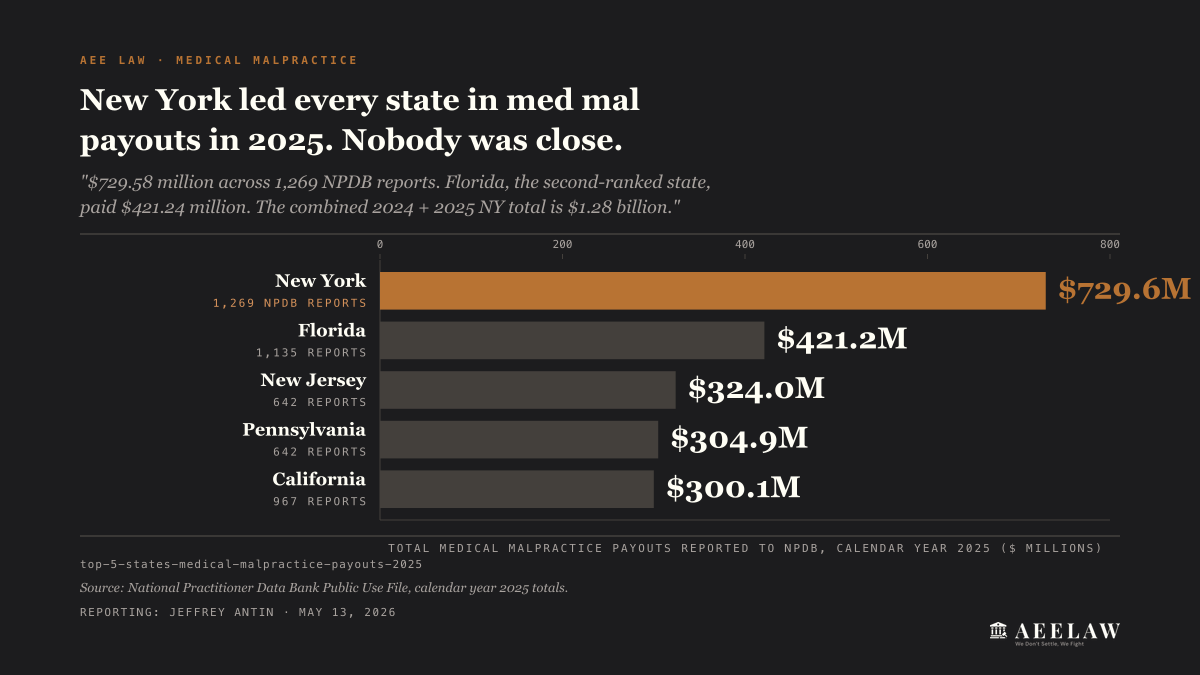
New York led every state in medical malpractice payouts in 2024 and 2025. The National Practitioner Data Bank logged $729.58 million across 1,269 reports in 2025, on top of $550.12 million across 1,205 reports in 2024.
That’s $1.28 billion in two years, spread across 2,474 NPDB-reportable payouts. Florida, New Jersey, Pennsylvania, and California round out the 2025 top five, and all trail New York.
Methodology
The state-level totals here come from the National Practitioner Data Bank Public Use File for calendar years 2024 and 2025. NPDB receives a mandatory report on every medical malpractice payment of $30,000 or more made on behalf of a licensed practitioner.
The sample frame is every reportable payment tagged to a New York-licensed practitioner with a New York primary practice address.
NYC Health + Hospitals payout data comes from the NYC Comptroller. The FY23 figures come from the published Annual Claims Report for fiscal year 2023.
The FY24 figure ($45.77 million) comes from the Comptroller’s Claims Dashboard, since the FY24 data publishes through that dashboard rather than a standalone report. Top-tier verdict figures come from TopVerdict.com and from published verdict reporting by NY plaintiff firms.
Two Years, Two Records
New York’s $729.58 million 2025 NPDB total broke the prior-year record by 33%. The 1,269 reports averaged out at roughly $570,000 per payout. Both numbers led the country.
The 2024 total of $550.12 million was already a national high. The 1,205 reports averaged out to about $456,000. Two years running, no other state came close.
The state-by-state gap is the part the headline misses. New York’s 2025 total led the next-ranked state by a comfortable margin. Florida, New Jersey, Pennsylvania, and California round out the top five, each well behind New York.
California and Florida, both larger by population, settle for less per state. New York’s combination of plaintiff-friendly liability rules, no statutory cap on non-economic damages, and a NYC jury pool drawn from five boroughs with the highest cost basis in the country produces a payout curve that flattens nowhere else.
NYC Health + Hospitals at $45.77 Million
Inside New York City, the public-hospital side of the story has its own number. NYC Health + Hospitals reported $45.77 million in tort claim settlements and judgments in fiscal year 2024, per the NYC Comptroller.
That made H+H the fifth-highest city agency, behind NYPD, the Department of Correction, the Department of Education, and the Department of Transportation. H+H operates 11 acute-care hospitals across the boroughs and serves more than a million patients a year, so the per-capita exposure runs differently from a private system.
The Comptroller’s FY23 report logged 398 medical malpractice claims filed against H+H, down 10% year-over-year, and $51.5 million paid across 64 resolved claims.
The FY24 number ($45.77 million) suggests continued moderation, though the long tail on med mal cases (most resolve five to ten years after the underlying care) means current-year claim filings won’t show up in current-year payouts.
H+H is one fraction of the citywide picture. The private side of New York’s hospital map (Mount Sinai, NYU Langone, NewYork-Presbyterian, Northwell, Montefiore, Maimonides) carries the majority of the city’s hospital-employed practitioner workforce, and the majority of the dollars passing through NPDB.
Where the Top-Tier Verdicts Come From
Top published New York medical malpractice outcomes in the recent reporting window run in the eight- and nine-figure range. Three examples from NY plaintiff-firm verdict pages and published reporting:
These cases are outliers, not the median. Most NY medical malpractice payouts resolve far below this tier. The verdict ceiling rides on three structural factors.
CPLR § 214-a sets the time window inside which a case has to land. New York places no statutory cap on non-economic damages. And NYC jury pools draw from boroughs with the country’s highest lost-wage and medical-care baselines. Severity of harm translates directly into damages.
What Lavern’s Law Changed
CPLR § 214-a(b), the Lavern’s Law amendment, took effect January 31, 2018. It applies to cancer and malignant-tumor diagnosis failures specifically. The clock for filing now runs from the date the patient discovered the missed diagnosis, or reasonably should have, with a seven-year outer cap measured from the date of the malpractice itself.
Before Lavern’s Law, the 2.5-year standard SOL ran from the date of the care. That structure routinely barred cases where a cancer was missed and not detected until years later, after the deadline had passed.
Lavern Wilkinson, the law’s namesake, died in 2013 of lung cancer that a Brooklyn hospital had failed to follow up on after an abnormal X-ray two years earlier. Her family could not sue because the SOL had already expired.
The 2018 amendment changes three rules for the cancer-misdiagnosis subset:
- Starts the SOL clock from discovery, not from the date of the missed diagnosis.
- Applies to acts of malpractice occurring on or after January 31, 2018. Pre-2018 misses don’t get the discovery rule.
- Caps the outer window at seven years from the date of the malpractice, so the rule isn’t open-ended.
For every other type of medical malpractice (surgical errors, anesthesia, OB-GYN injuries outside cancer misdiagnosis, ER misdiagnosis of non-cancer conditions, medication errors), the standard 2.5-year clock under CPLR § 214-a still controls. Continuous treatment can toll the clock in some circumstances, and minors’ rights are preserved separately under CPLR § 208.
The Hospital Concentration Question
The five-hospital-systems hypothesis (that a handful of NYC systems carry most of the med mal volume) is plausible on its face. NYC’s private hospital market is dominated by a small number of large multi-hospital systems, and procedure volume concentrates inside them. But the public data doesn’t answer the concentration question directly.
NPDB tags by practitioner. A payout in a Mount Sinai cardiac surgery case is reported against the operating cardiac surgeon’s record, not against Mount Sinai’s.
Hospital-system attribution requires a separate cross-walk: pulling the practitioner’s primary affiliation from the NY State Department of Health profile, joining it to the NPDB record on the practitioner’s NPI or license number, then aggregating dollars per hospital system. That join is buildable but not built into the NPDB Public Use File release.
The closest publicly available proxy today is the NYC Comptroller’s H+H claims data ($45.77 million in FY24) combined with TopVerdict.com’s individual hospital-named verdicts and published verdict reports from NY plaintiff firms. None of that gets you to a clean hospital-system ranking.
A complete picture would require the NPDB-to-DOH-Profile cross-walk plus a TopVerdict-to-Comptroller-to-private-insurer-disclosure merge that no single public file supports today.
The hospital concentration map is the next data move on this beat.
What This Means for People Injured by NYC Hospital Care
If you were hurt by hospital care in NYC, three points the data above changes:
The dollar exposure is real. New York’s national lead in med mal payouts, two years running, means insurers and self-insured systems carry capacity for large settlements when liability is clear. The $570,000 average across 1,269 NPDB reports in 2025 reflects what actually resolves, not what gets demanded.
The deadline is the trap. The 2.5-year clock under CPLR § 214-a is one of the shorter SOLs in the country.
Many cases that would survive in California (three years) or Florida (two years from discovery, four-year cap) die in New York because the clock starts at the care, not at the discovery. The cancer-misdiagnosis exception under Lavern’s Law is the only carve-out, and it applies only to cancer cases.
NYC Health + Hospitals settles differently than private systems. H+H is the city’s public hospital network, and tort claims against it run through the Comptroller’s claims process with notice-of-claim requirements under NY GML § 50-e.
The 90-day notice deadline is shorter than the underlying SOL, and missing it is the most common preventable error in public-hospital med mal cases.
Hospitals settle quickly when a case is built for trial.


