
NYC Health + Hospitals runs 11 acute care hospitals. Together they resolved 61 medical malpractice claims for $44.9 million in fiscal year 2023, and they took 347 new claims the same year. The Comptroller publishes every facility name. The State Health Department publishes the inspection record. CMS publishes the fall and pressure-ulcer rates. Nobody publishes the cross-walk a patient would need to read all three together.
Methodology
Facility-level claims and payout data come from the NYC Comptroller’s Annual Claims Report for fiscal year 2023, released April 16, 2024. Table 4 of that report breaks out all 11 NYC Health + Hospitals acute care facilities by name: Bellevue, Coney Island, Elmhurst, Harlem, Jacobi, Kings County, Lincoln, Metropolitan, North Central Bronx, Queens Hospital Center, and Woodhull. The $44.9 million / 61 claims resolved / 347 claims filed figures are the Table 4 totals across all 11. This analysis highlights the seven highest-payout facilities. “Claims resolved” counts cases closed in FY23, whether by settlement or judgment. “Claims filed” counts new cases initiated in FY23. The system-wide H+H total of $54.5 million in tort claim payouts comes from the same Comptroller release.
The fall and pressure-ulcer measure rates referenced here are publicly available through CMS Care Compare and the CMS Provider Data Catalog, joined to NYS Department of Health Hospital Profiles inspection records. We treat the cross-walk between Comptroller payout dollars, NYS DOH inspection deficiencies, and CMS quality measures as the open editorial question. No public agency publishes that join.
What the Comptroller Actually Published
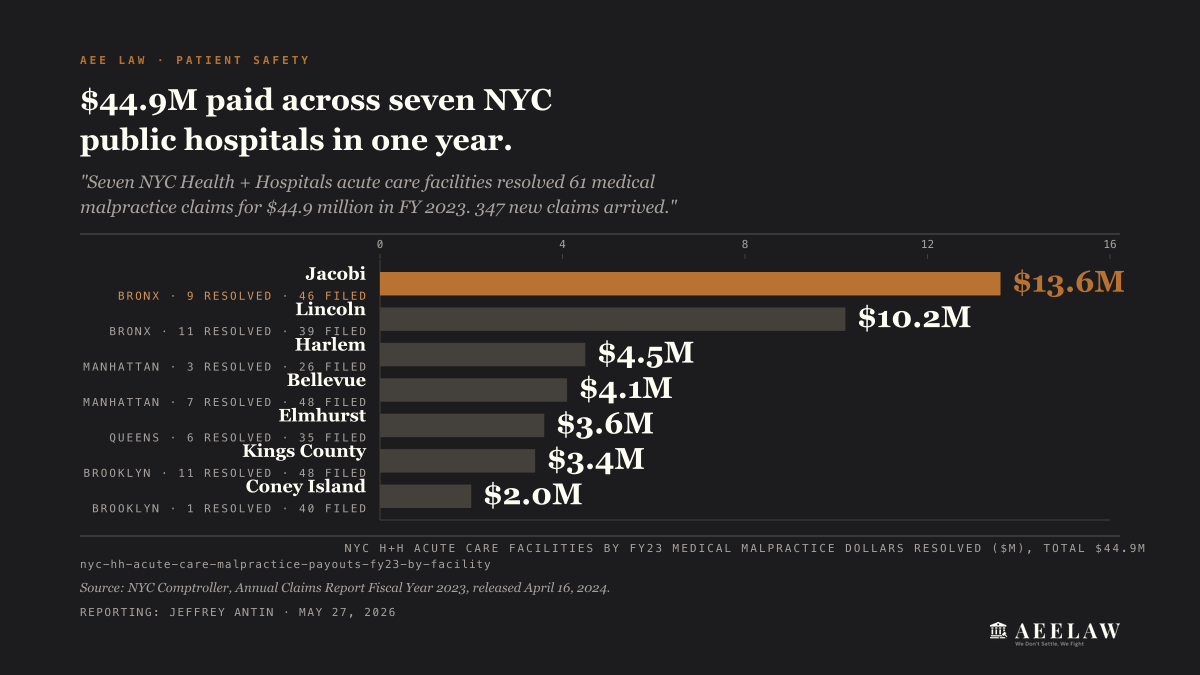
The Comptroller’s FY23 report names all 11 H+H acute care hospitals and itemizes each one’s FY23 numbers. Here are the seven that paid out the most. Jacobi, the system’s Bronx flagship, resolved 9 medical malpractice claims for $13.6 million, with 46 new claims arriving that year. Lincoln, the South Bronx Level I trauma center, resolved 11 claims for $10.2 million on 39 new filings. Harlem closed 3 claims for $4.5 million on 26 new. Bellevue closed 7 claims for $4.1 million on 48 new. Elmhurst, Queens, closed 6 for $3.6 million on 35 new. Kings County, Brooklyn, closed 11 claims for $3.4 million on 48 new. Coney Island closed 1 claim for $2.0 million on 40 new.
The two top dollars (Jacobi at $13.6M and Lincoln at $10.2M) are both Bronx hospitals. The two largest new-claim volumes (Bellevue and Kings County, 48 each) tie one Manhattan facility to one Brooklyn facility. The seven hospitals above carry $41.4 million of the malpractice dollars. The other four acute care hospitals (Metropolitan, Woodhull, Queens Hospital Center, and North Central Bronx) carry the rest, for an 11-hospital total of $44.9 million on 61 claims resolved. The H+H system as a whole paid $54.5 million in tort claim settlements and judgments in FY23, down from $82.7 million in FY22.
That’s the number a patient or a reporter can quote from the Comptroller release. The question of how those dollars distribute by clinical harm category (falls, pressure ulcers, surgical error, ER delay, medication error) is not in the public release. The Comptroller files settlements at the claim level, not at the harm-category level.
What the State and CMS Publish Separately
The NY State Department of Health maintains a public Hospital Profile for every licensed acute care hospital in New York, accessible at profiles.health.ny.gov. The profile carries the inspection history, including Statements of Deficiencies issued during NYSDOH surveys. A fall on an inpatient unit that produces a serious injury can produce a citation in the next survey cycle. So can a stage III or IV pressure ulcer that hospital staff failed to prevent or document. The deficiency text is public. The aggregate count across facilities is not published in a sortable cross-facility format.
CMS publishes per-facility quality measures through Care Compare and the Provider Data Catalog. The measures include the long-stay fall-with-major-injury rate for skilled-nursing facilities, the pressure-ulcer rate for high-risk long-stay residents, and the hospital patient safety indicators for inpatient units. Joining these CMS measures to the NYS DOH inspection record produces a per-facility clinical-harm profile. Joining that to the Comptroller’s facility-level dollars paid produces the cross-walk patients need.
The three datasets sit in three separate publishing pipelines. No agency joins them. The data has been public for years.
CMS Just Made Falls the Priority Signal
On January 28, 2026, CMS issued updates to the Nursing Home Special Focus Facility (SFF) program. The new methodology instructs state survey agencies to consider the prevalence of falls when selecting nursing homes from the SFF candidate list. CMS also tightened the inspection cadence: standard health inspections at SFFs will now run at least once every six months, with Life Safety Code and Emergency Preparedness surveys at least annually. The candidate-list lookback narrows from the past three standard surveys to the past two.
For NYC, the change matters in two ways. First, a nursing home flagged under the new methodology is a facility whose federal regulator has named falls as a serious concern. That is admissible notice of risk in any subsequent injury case. Second, the SFF designation accelerates the federal inspection pipeline, which in turn produces more documented deficiencies in the NYSDOH record, which in turn feeds back into the evidence base for future malpractice claims.
ProPublica’s Nursing Home Inspect tool tracks the federal deficiency record, and it updates as new surveys post. Grand Manor Nursing & Rehabilitation Center in the Bronx is one NYC example. CMS lists Grand Manor as a Special Focus Facility, its survey history runs to dozens of deficiencies since 2021, and federal fines against it total more than $327,000 over three years. The flag is the pattern, not any single citation. A facility that the federal program has already singled out for extra scrutiny is a facility whose own regulator has documented the risk in writing. That documentation is the editorial signal.
The Two Statutes That Close the Door Fast
Two New York statutes close the legal window on public-hospital cases faster than most patients realize.
GML § 50-e, the 90-day Notice of Claim rule. NY GML § 50-e requires anyone planning to sue a public corporation, including the 11 hospitals run by NYC Health + Hospitals, to serve a sworn written Notice of Claim within 90 days of when the claim arose. The notice must name the claimant, describe how and when the claim arose, and itemize damages. The statute reads: “the notice of claim shall comply with and be served in accordance with the provisions of this section within ninety days after the claim arises.”
Miss the deadline and the case is generally barred, even when the underlying malpractice is well documented. The rule applies to Jacobi, Lincoln, Harlem, Elmhurst, Bellevue, Kings County, Coney Island, Metropolitan, Woodhull, Queens Hospital Center, and North Central Bronx. Most patients do not learn which hospitals are public until after discharge.
CPLR § 214-a, the 2.5-year statute of limitations. Under CPLR § 214-a, the general statute of limitations for medical malpractice in New York is two years and six months from the act or omission, or from the end of continuous treatment for the same condition by the same provider. The statute reads: “An action for medical, dental or podiatric malpractice must be commenced within two years and six months of the act, omission or failure complained of.”
Lavern’s Law, the 2018 amendment, adds a discovery rule for cancer and malignant-tumor misdiagnosis cases, with a seven-year outer cap. Falls and pressure-ulcer cases run on the standard 2.5-year clock. For a patient hurt at an H+H hospital, the 90-day Notice of Claim deadline sits on top of the 2.5-year SOL, and the shorter one controls in practice.
The combination is the operational trap. A patient injured at Bellevue in March knows by April that something went wrong, but does not learn until later that Bellevue is a public hospital subject to the 90-day rule. By July, the Notice of Claim window has closed.
What This Means
Three takeaways:
The named facilities are public. The Comptroller publishes all 11 acute care hospitals by name in the FY23 claims report, with line items for claims resolved, dollars paid, and new claims filed. Jacobi, Lincoln, Harlem, Bellevue, Elmhurst, Kings County, and Coney Island paid out the most. Any patient, family member, or reporter can pull the PDF off the Comptroller’s site today. The cross-walk to clinical harm categories like falls and pressure ulcers is the next data move.
The data gap is the story. NYC publishes the dollars. New York State publishes the inspections. CMS publishes the quality measures. No single agency publishes the join. A Bronx patient choosing between Jacobi and Lincoln cannot see whether the hospital with the worse inspection record is also the hospital paying out more settlements. The three datasets sit in three separate publishing pipelines, and a determined patient has to build the comparison from scratch.
The clock starts at the harm, not the discovery. For a fall or a pressure ulcer at an H+H hospital, GML § 50-e’s 90-day Notice of Claim deadline runs from the date of the harm, not from the date the patient learns the hospital is public. The 2.5-year SOL under CPLR § 214-a runs on the same clock. Patients who wait to file because they’re still in the hospital, still recovering, or still hoping the facility will resolve the complaint internally generally find both clocks already running.
The Comptroller knows. The State knows. CMS knows. The patient still has to build the map.


